Group Method for Large-Scale Testing, Applicable to the COVID-19 Coronavirus, SARS-CoV-2
Boris Conforty, March 25th 2020Updated March 31st
PDF version of this article | Automatic translation
Abstract
In response to the rapid spread of COVID-19, testing as many people as possible has been widely advised by experts and international organizations. Advice and policies have later changed to a much more targetted testing, of symptomatic patients or persons at risk for instance. This shift was caused by the number of available test kits, by far lower than what would be needed to test extensively. As a result, alternative strategies to contain the spread of the pandemic have been put in place around the world, with extreme restrictions, impacting both private life and the economy to an extent unseen in peacetime. In the event of massive spread of COVID-19 in developing countries, where intensive care facilities are less readily available than in developed nations, healthcare systems would face enormous challenges.
In this article, I present a study of an optimized testing protocol, which can produce a multifold increase in the number of people tested (e.g. 5-6x when incidence rate is 1%, 35x when incidence rate is 0.1%). The handling of the pandemic – and the associated fatalities and economic difficulties – could change dramatically as a result.
Content
- Context: test, test, test
- Insufficient test kits for COVID-19
- Current testing methodology
- Proposed methodology – Group testing
- Feasibility
- Simulations
- Conclusion
Context: test, test, test
March 16, WHO's Director-General tweeted: "We have a simple message for all countries fighting #COVID19: test, test, test.":
We have a simple message for all countries fighting #COVID19: test, test, test.
— Tedros Adhanom Ghebreyesus (@DrTedros) March 16, 2020
The most effective way to prevent #coronavirus infections and save lives is breaking the chains of transmission. And to do that, you must test and isolate. https://t.co/cOOs5wMCZE
Academics around the world have called for testing to be scaled up:
More information about the context of the coronavirus disease (COVID-19) pandemic can be found here:
- WHO's (World Health Organization) website
- Wikipedia - 2019–20 coronavirus pandemic
- Wikipedia - Coronavirus disease 2019
Insufficient test kits for COVID-19
It has become obvious that test kits will not be in sufficient supply to test at large scale. For that reason, recommendations are now commonly to test symptomatic or vulnerable persons only.
"Due to limited testing, as of March 2020, no countries had reliable data on the prevalence of the virus in their population. This variability also affects reported case-fatality rates." (Wikipedia)
The reality is that extensive testing with the current methodology is not possible. On March 23, WHO's Director-General advised "targeted tactics" and "testing every suspected case" only:
To win, we need to attack the virus with aggressive and targeted tactics – testing every suspected case, isolating and caring for every confirmed case, and tracing and quarantining every close contact.
— Tedros Adhanom Ghebreyesus (@DrTedros) March 23, 2020
This is currently the targeted, limited testing policy applied by all countries under acute pandemic pressure. A case can only be confirmed after the patient has symptoms, presumably long after he or she has become contagious.
More information:
Current testing methodology
Even if the technology is advanced, methodology is rather simple: if an individual fits the testing selection policy, a biological sample (nasopharyngeal swab or sputum sample) is taken and a test (RT-PCR) is performed to detect viral genetic material.
Results are ready in as little as a few hours.
One kit is used to test one individual.
One million kits are required to test one million individuals.
Proposed methodology – Group testing
I propose here a method to significantly reduce the number of test kits required whenever the incidence of expected positive results does not exceed 15% (see "Influence of disease incidence rate" below for why).
Test groups of people – instead of individuals – with one kit per group.
Testing a group means mixing their samples and treating them temporarily as one sample.
Several rounds of testing progressively smaller subgroups can be required for groups tested positive.
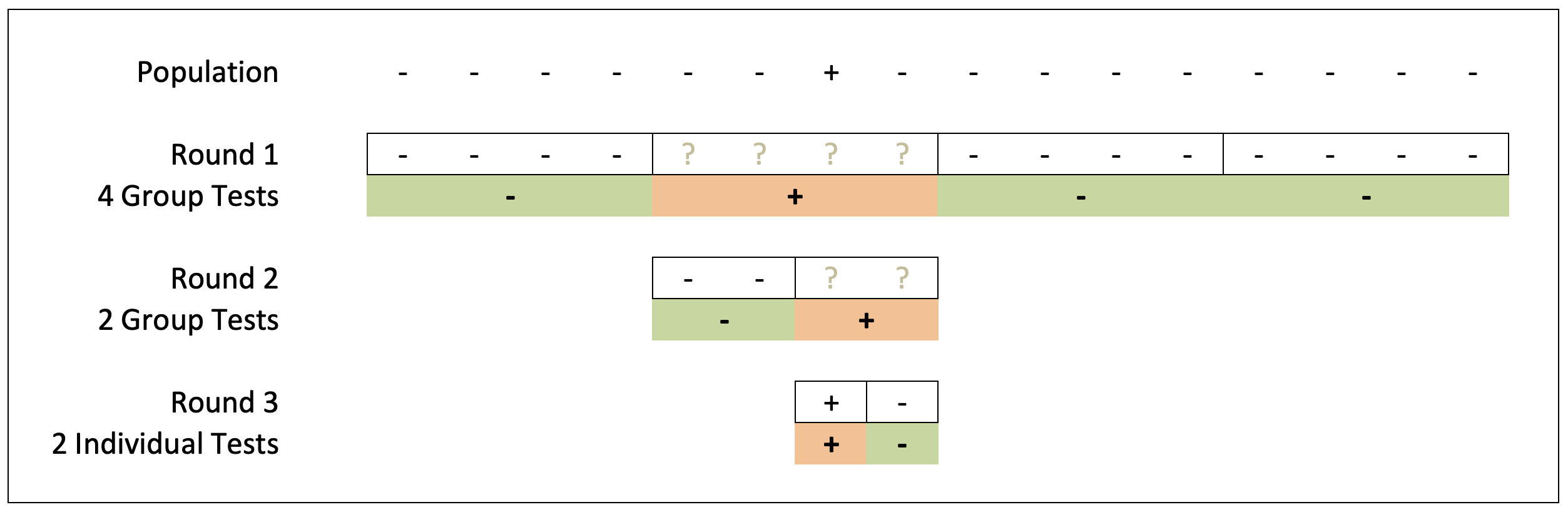
In this example, a population of 16 individuals, where 1 is infected, requires 8 test kits to test all 16 individuals instead of 16 kits. Groups of 4 were used as a starting point.
Group testing allows testing many more individuals than the standard protocol. Note that this strategy can be applied to any test, and is not specific to the current COVID-19 RT-PCR screening.
More information (thanks to Oleg Aseev for mentioning a similar – or even identical – theory):
Best case scenario
Since the test is binary (the result is either positive or negative), a group where nobody is positive will give a negative result. That is the best case, assuming the test is fully reliable, where one test kit only is necessary to test all individuals in the group.
Other scenarios
A group where at least one individual is positive will give a positive result.
In that case, and if testing kits are in short supply, the policy could be to quarantine or isolate all members of that group.
If more test kits are available, and since the goal is to diagnose infected individuals, the group should further be split into two groups, with a new test performed on each group. That could prove sufficient, or a new round of testing with even smaller groups could be decided, until groups contain single individuals only.
Remember that as soon as a group tests negative, further testing for its members is not required.
Feasibility
One might wonder if this is feasible in practice, in the context of COVID-19 testing. It seems so, since a test takes a few hours, biological samples can be stored for weeks for reuse, and at least a few biological samples can be mixed together for group testing (thanks to Virginie Peter and Claire Bertelli for their input on this). Confirmation by people with experience with COVID-19 testing would be appreciated.
Update: A study (by Israel Institute of Technology and Rambam Health Care Campus) published on March 27 shows that "Detection of positive samples diluted in even up to 64 samples may also be attainable, though may require additional amplification cycles. As it uses the standard protocols, reagents and equipment, this pooling method can be applied immediately in current clinical testing laboratories".
Simulations
I performed simulations to estimate the number of tests needed to screen populations with specific incidences of positive individuals.
Variables are:
- Population size, fixed at 1 million for the purpose of this study
- Incidence rate of positive individuals
- Size of test groups at the beginning of the screening (limited to powers of 2, i.e. 1, 2, 4, 8, 16,...)
Output is:
- Number of tests performed
At each run, a population is randomly generated, where individuals are either negative or positive and have a probability to be positive equal to the incidence rate.
Then individuals are grouped and each group is tested. Every group with a positive result is further split and subgroups are tested. Groups with a negative result confirm that their members were all negative and no further testing is needed for these individuals.
JavaScript code is available upon request.
When the incidence rate of positive cases is 1%
Here is the total number of tests required to test every individual as a function of group size. The simulation was done with an incidence of positive individuals of 1%:

The curve showing an optimal group size of 16 or 32, with fewer than 200'000 tests needed to test the whole population of 1 million individuals.
To put things into perspective, in these conditions, testing the whole population of Switzerland (8.5 million) would require fewer than 2 million test kits. To test the whole US population (328 million), around 70 million kits would be enough. I'll show below that these numbers depend greatly on the actual infection incidence, and could be dramatically lower if testing is done before the incidence rate reaches 1%.
Another way to show this result is by plotting how many individuals can be tested with 1 million kits:

One million test kits can be used to test almost 6 million individuals.
Influence of disease incidence rate
The lower the incidence rate, the more individuals a single kit can test (scales are logarithmic):

When incidence rate is 0.1%, it is possible to test more than 35 individuals with a single test kit, if done at a large scale.
Influence of variations of incidence in subpopulations
Clearly, there are many ways to optimize this protocol, and to adapt it to the current crisis or to any future epidemic or pandemic.
For instance, the number of required test kits can be brought down by splitting the population into subpopulations. Data for COVID-19 suggests that children might be less likely to get infected by SARS-CoV-2. A single test could thus on average test more children than adults.
Conclusion
This work shows that group testing for COVID-19 could radically change the way we track the spread of the infection in populations. Good tracking has been shown to be key in keeping the spread of an epidemic, or a pandemic, under control. Given the past situation in Asia, the current situation in Europe and the USA, and maybe even more given the much-feared expansion to Africa and developing countries in general, I strongly advise re-examination of the testing protocols enforced by governments, and of advice provided by international organizations.
Updates
- March 31: Added text and link about feasibility study
Acknowledgments
I would like to thank:
- Prof. Andras Szenes, Geneva University, Switzerland
- Oleg Aseev, PhD, MIRO Analytical, Zurich, Switzerland
- Djilani Kebaili, EPFL, Geneva, Switzerland
for their comments and suggestions, and
- Claire Bertelli, PhD, Lausanne University, Switzerland
- Virginie Peter, Lausanne University, Switzerland
for providing useful information about RT-PCR.
Author
Boris Conforty, EPFL, Geneva, Switzerland